CASE REPORT
An asymptomatic 63-year-old woman attended for her first screen as part of the National Health Service Breast Screening Programme. Mammograms showed involuted breasts with a 20mm, well defined opacity in the lower inner quadrant of her left breast (Fig. 1). The opacity contained fine punctate microcalcification and localized compression views demonstrated a halo, suggesting it was benign. Although the patient was unaware of its presence the mass was palpable as a smooth, well defined lesion. Ultrasound examination showed a well defined, solid, mainly hypoechoic lesion containing small, bright echoes consistent with areas of calcification (Fig. 2).
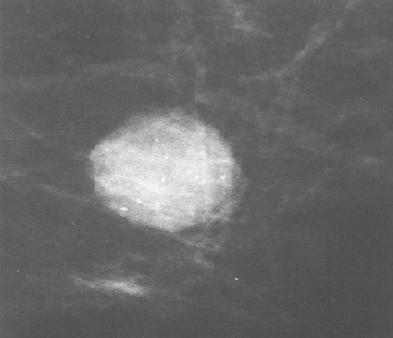
Fig. 1 - Magnified view of the 20 mm lesion in the lower half of the left
breast, showing its well defined margins and microcalcification within it.
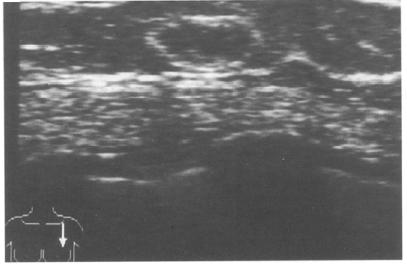
Fig. 2 - Ultrasound image of the well defined mass
Although the mass was thought most likely to represent a benign lesion such as a fibroadenoma, the fine microcalcifications within it were considered to be atypical and surgical excision was recommended. Fine needle aspiration cytology was not available at the time of presentation. Naked eye inspection of the excised specimen revealed a dark red, well circumscribed mass measuring 20 x 15 x 15mm which exuded blood from its cut surface. Specimen radiography showed the microcalcification confirming the lesion's removal but, the radiodensity of the mass was much less obvious than on the screening films (Fig. 3).
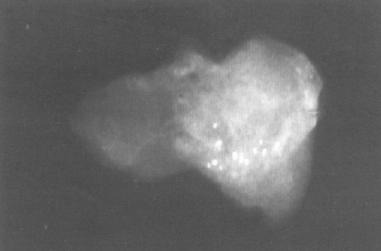
Fig. 3 - Specimen radiography of the excised lesion showing the
calcifications. The mass itself is not at all obvious.
On histological examination the lesion was found to be a haemangioma. Some of the vascular spaces within it contained calcifed thrombus (Fig. 4).

Fig. 4 - Histological section of the haemangioma. The arrow indicates the calcified thrombus.
DISCUSSION
Haemangiomas of the breast are benign vascular tumours and although they are characteristically erilobutar in location, they can occur both within and beyond lobular units [1]. One study of post mortem specimens of the female breast found the incidence of perilobular haemangioma to be 11%, however, all of these lesions were small, none being greater than 4 mm [2]. Our case is unusual because of its size. Indeed, palpable vascular tumours of the breast are likely to be angiosarcomas rather than haemangiomas [3]. The mammographic appearances of haemangiomas have been previously illustrated by Tabar and Dean who describe two cases. One case was similar to ours[4], with a well defined, lobulated mass showing fine microcalcification. The second lesion was well defined, lobulated and also showed calcification, but the calcification was much coarser and bizarre in appearance [5].
We have only found one previous report documenting the ultrasound appearances of breast haemangioma [6].In contrast to our findings, that lesion was a poorly defined hyperechoic mass which showed marked distal attenuation.
Colour Doppler ultrasound has been used in the diagnosis of perilobular haemangioma which was causing repeated bleeding from the nipple in a 14-year-old girl [7]. Mammograms in that patient were normal.A further feature of note in our case is the reduction in radiodensity of the lesion on specimen radiography, presumably because it no longer contained blood. This alteration in density on specimen radiography has not previously been described and could mislead the surgeon into believing tha t the excision had been unsuccessful. In this case, the presence of the venous calcification within the specimen enabled us to confirm radiologically that the lesion had been successfully excised.
REFERENCES
1 Nielsen B. Haemangiomas of the Breast. Pathological Research Practice 1983;176:253-257.
2 Leseuer GC, Brown RW, Bhathal PS. Incidence of Perilobular Haemangioma in the Female Breast. Archives Pathological Medicine 1983;107:308 310.
3 Sebek BA. Cavernous Haemangioma of the Female Breast. Cleveland Clinic Quarterly 1984;51:471 474.
4 Tabar L, Dean PB. Teaching Atlas of Mammography, 2nd edn. New York:George Thieme Verlag Stuttgart, 1985:45.
5 Tabar L, Dean PB. Teaching Atlas of Mammography, 2nd edn. New York: George Thieme Verlag Stuttgart, 1985:209.
6 Guyer PB, Dewbury KC. Sonomammography. An Atlas of Comparative Breast Ultrasound. John Wiley and Sons, 1987:139.
7 Gembala RB, Hayward CZ, Ball DS et al. Colour Doppler Detection of a Breast Perilobular Haemangioma. Journal of Ultrasound in Medicine 1993;4:220-222.
.com>
 典型病例分享
典型病例分享